
1. Thinking back on some of the communications issues in the United States that surfaced during the flu pandemic, what were some of the main challenges?
One of the biggest communication challenges was trying to keep policies and messages up to date as the experts’ knowledge evolved. Just as important was letting the public know that this would happen – forewarning people to expect that policies and messages would change as the data and the situation changed. It is very difficult to meet these twin challenges successfully. More often than not, U.S. officials failed to do so. Sometimes they didn’t seem to try.
The CDC started out beautifully. On April 24, at the start of his second swine flu press briefing as acting CDC director, Richard Besser said explicitly: “Our recommendations, advice, approaches will likely change as we learn more about the virus and we learn more about its transmission….”
But the message of uncertainty and unpredictability wasn’t emphasized nearly often enough. With regard to vaccine availability and efficacy, for example, officials were insufficiently clear that they couldn’t tell how soon there would be enough vaccine or how well it would work against the virus. Nor did they stress sufficiently their inability to predict how severe the pandemic would be, how widespread it would be, or how quickly it would peak and decline. As these factors played out, the U.S. ended up with a vaccine shortage when the demand was strongest and a surplus after the demand waned. It would have been helpful if the public had understood more clearly that this was among the possibilities – one of many possibilities – from the outset.
Sometimes officials followed through on Dr. Besser’s promise to change policies as the data and the situation changed. For example, the CDC’s recommendations about school closure changed early in the pandemic. This resulted in some short-lived but certainly unfair criticism suggesting that the changes reflected CDC inconsistency or incompetence. Perhaps that criticism discouraged the agency from being similarly candid about other changes as knowledge about the pandemic (and the pandemic itself) evolved.
A key example: As age-specific risk data evolved, showing for instance that people 65 and older had a higher death rate than children, and showing that people 50–64 had the highest death rate of any age group, the messages based on earlier data did not change. The old messages were re-emphasized over and over: “Children and young adults are most at risk. Get your children vaccinated. Young adults, get vaccinated!”
When the CDC’s Advisory Committee on Immunization Practices discussed its priority group recommendations in the summer of 2009, the committee was explicit about the possibility that the data on which its recommendations were based might change. At the July 29, 2009 ACIP meeting, the chair of the Influenza Vaccine Work Group, Kathy Neuzil, emphasized that the committee must: “Recognize and acknowledge uncertainties, as well as the potential need to reconsider recommendations as more data become available.”
Long before the H1N1 vaccine became available, data began to show that children and young adults were less at risk from the pandemic than older people, though still more at risk from the pandemic than from the average seasonal flu. The new information was not stressed by U.S. health officials. Much of the messaging, in fact, strongly implied that children and young adults were more at risk than older people. The public was never made aware of what Kathy Neuzil had called “the potential need to reconsider recommendations as more data become available.”
It is likely that the public would have wished the priorities to remain the same despite the new data. Most surveys show a strong desire to protect children and young people first. But the public never had a real opportunity to consider the question.
2. With the virus turning out to be less severe than first thought, how did the risk message evolve over the first year of the pandemic?
Even the way you ask the question – “with the virus turning out to be less severe than first thought” – signals that officials initially over-confidently signaled their fears that the pandemic was really bad. Prior to April 2009, virtually all officials did fear that “the next pandemic” would be at least as bad as 1957. With bird flu on their minds, most were imagining a pandemic much worse than 1957.
So the initial terrifying impression from Mexico was the understandable starting point. But it very quickly became clear that in its early phase of global transmission, H1N1 was a very low-mortality strain of flu. Yes, it caused an increase in the usually very low mortality rate in people under 65, but it caused a drastic decrease in the usually very high mortality in the elderly. (The elderly still died at a higher rate than children.)
The single biggest severity messaging problem was the failure of officials to stand down convincingly from their initial fears. Because the H1N1 pandemic was killing more children than seasonal flu, it became anathema to call the pandemic “mild.” In the past, the CDC has routinely labeled certain seasonal flu years as “mild,” “mild to moderate,” etc. And public health officials have routinely called the 1968 pandemic “mild” or “relatively mild.”
The failure to call the evolving pandemic “mild so far” didn’t mislead people about its mildness. People figured out without much help from officials that the pandemic was mild so far. But many ended up perplexed and even skeptical about why officials weren’t saying so. This skepticism was far less pronounced in the U.S. than in Europe, where some editorialists and parliamentarians accused the World Health Organization of promulgating a “fake pandemic.” But it was a problem even in the U.S.
And it remains a liability as we look ahead to future public health threats. If officials are unwilling to call a mild flu virus mild, they lose some of their ability to warn convincingly that a mild flu virus can turn severe at any point.
We are not saying that officials overstated the seriousness of the pandemic risk. If anything, they understated the potential risk. The experts we talked with were much more worried about H1N1 in the early days than their public statements acknowledged. They are much more worried about H5N1 now than their public statements acknowledge.
That’s the challenge: to help the public understand that what might have happened and might still happen is really, really awful, and simultaneously to help the public understand that what has happened so far is a huge relief and a bit of an anticlimax … that what has happened so far isn’t what officials have been worried about and warning about.
Today, officials are having a tough time convincing the public that the H1N1 threat is not over. Having failed to acknowledge that the pandemic is pretty mild so far, they can’t find the words to explain that it could come back worse. “Pretty mild so far but could come back worse” is a message that might have encouraged more interest in post-second-wave vaccination. “Pretty mild so far but could come back worse” is what propelled the two of us to get our H1N1 vaccinations as soon as we were eligible – in January 2010, after the second wave. But that was our own message to ourselves, not the message that came from officials.
3. Federal officials had a lot on their plate, pitching two vaccines to different risk groups that didn't quite match up. How did the message surrounding vaccination change over the course of the first year?
We’ll pass on answering this one.
4. Parents seemed eager to vaccinate their kids, but uptake in adults seemed disappointingly low, as opinion polls showed many thought they weren't at risk. What do you think contributed to that?
Officials systematically overstated the risk to young people, especially kids, and understated the risk to older people. The early meme that older people seemed to have some pre-existing immunity persisted even as their population death rates quickly grew, equaling (65+) or exceeding (50–64) the death rates in younger groups.
Look at all the links to HHS public service announcements on the flu.gov website: page after page emphasizing the need for vaccination in children, young adults, and pregnant women. There weren’t even any PSAs targeting high-risk 50–64-year-olds, even though that group was on the list of official priority groups. By far the strongest message emanating from HHS, at least until after the second wave ended, was that young people should get vaccinated.
Lots of doctors we know said they didn’t push H1N1 shots to their older patients because “older people were much less at risk.” This is despite the fact that all adults aged 25–64 with high-risk conditions were a priority group for early vaccination. Of course, doctors were told not to vaccinate their elderly patients at all, until there was a vaccine surplus.
In short, HHS, the CDC, and all the local health officials who followed their lead overemphasized the risk of H1N1 to children and young adults at the cost of underemphasizing the risk to older adults and seniors – a decision made in the face of knowledge that adults 50–64 had the highest death rate, and that seniors’ death rate was about the same as the rate for people 25–49. Officials leaned on the truth that swine flu was far deadlier to the young than seasonal flu to imply the falsehood that it was deadlier to the young than to older people.
Officials got what they asked for. Grandparents pushed their children to vaccinate their grandchildren, and neither parents nor grandparents thought it was necessary to get vaccinated themselves. If the vaccine had been available sooner or the pandemic had lasted longer, this approach would have saved some lives of children and cost more lives of older people. As it turned out, the vaccine arrived when the 2009 pandemic was already waning, so these targeting decisions had very little actual health impact.
5. How effective was the messaging regarding vaccine safety?
U.S. officials did an extremely good job of acknowledging that there were widespread doubts about the safety of the swine flu vaccine. They wisely refrained from pushing too hard. Vaccination was voluntary, not required; people were urged to make up their own minds, and were given “permission” to watch and wait until they felt sufficiently confident that no serious vaccine safety problems had emerged. (The comparative mildness of the pandemic and the delay in vaccine availability made this an easy decision.) We never felt that officials were implying it was foolish to worry about the safety of the vaccine. Officials said the vaccine was safe, but they didn’t say worrying about it was stupid.
Officials also developed an impressive program to track claims of adverse events and to assess whether there were more such claims than could be accounted for by coincidence. These confidence-building measures were aimed more at physicians and the general public than at anti-vaccination activists. Dedicated opponents probably couldn’t have been won over anyway, but it might have helped persuade some mildly mistrustful skeptics if there had been more effort to involve people who weren’t closely tied to the pro-vaccination public health establishment.
Despite this “fox guarding the henhouse” aspect, on the whole vaccine safety messaging was good. Of course it’s impossible to know how well the messaging would have been handled if potentially serious vaccine safety issues had arisen.
6. What are some of the main lessons public health officials learned in communicating about the pandemic, the vaccine, and antivirals?
We don’t know yet if public health officials have learned many communications lessons. We fear that top officials may have mislearned some lessons. They may have “learned” that they can get away with misleading the public without getting caught. So far, the CDC hasn’t gotten into any trouble for overstating the danger to people under 25 and understating the danger to older people, especially the most endangered 50-to-64-year-old age group.
We are also afraid that officials may have mislearned the lesson that it is the media’s fault (and now of course that includes the social media) when the public misunderstands or rejects official messages. It is harder to work on improving your own communication strategies when you outsource the blame instead of owning the blame.
We hope officials have learned not to make overconfident promises about vaccine availability and efficacy. We hope they write some boilerplate messages right now about how uncertain and unpredictable flu vaccine production and efficacy are. And we hope they write a note to themselves to repeat those messages over and over, both in pandemics and in regular flu seasons.
We wish officials would stop exaggerating the flu-preventing benefits of hand-washing and cough hygiene. Instead, officials should acknowledge that these are important measures that might help a little; that they are better than nothing; and that they are relatively easy to implement, inexpensive, and under your own control in your daily life during a pandemic.
And we wish officials would stop implying that their efforts to fight the H1N1 pandemic have already paid big dividends. Hand-washing and cough etiquette helped only a little because a little is all they can help. Vaccination helped only a little because there was sufficient vaccine only when the second wave was already waning. We lucked out with a mild pandemic so far.
We hope officials have learned not to imply that “everyone who needs it” will be able to get antivirals from their doctors as soon as the need arises, and that there is therefore no value to personal antiviral stockpiles. During the pandemic, the CDC discouraged low-risk patients from seeking medical attention early in their illness unless their symptoms were severe. And the CDC discouraged doctors from giving low-risk patients Tamiflu early in their illness when it works the best, despite data that a significant percentage of those who eventually developed serious illness were in low-risk groups. We keep Tamiflu at home, and we urge our friends to do the same. (We stockpiled it at a time when demand was low.)
All of these wishes are in the service of our hope that officials will learn to communicate in ways that are more trustworthy.
7. Are there some notable successes that health officials will be able to use in preparing for the next big disease threat?
Despite the appearance of chaos in the H1N1 vaccine roll-out, U.S. officials organized the delivery and administration of vaccine almost as quickly as it was produced, starting with six million doses just before the peak of the second wave. This required amazing operational communication, as well as communication with the public.
CDC Director Tom Frieden tried hard to communicate the “bumpy road ahead” message during the initial rollout, and this should be a message that gets shouted from the rooftops in future crises. Unfortunately, Frieden was undercut by overpromising vaccine messages from HHS officials, which predictably generated public and political outrage when the vaccine failed to arrive on schedule.
It would help, but only a little, to emphasize that “bumpy roads” that look chaotic are sometimes actually signs of resilience and adaptability – but to acknowledge that it can still feel like chaos to the public.
8. The pandemic seemed to emerge just as social networking tools were hitting the mainstream. What role did they seem to play?
Lots of flu pandemic social networking tools were active for several years before H1N1 emerged, and the most impactful ones like Flu Wiki played an important role in raising awareness, which helped spur preparedness efforts.
Before and during the pandemic, public health blogs that were perceived as highly trustworthy and articulate, such as Effect Measure, became important sources for reporters, officials at all levels, and the interested public as well.
Of course the ratio of wacko to responsible social networking sites increased dramatically after the pandemic emerged. Anyone with an ax to grind could find reinforcement at sites that matched his or her viewpoint. People who were worried about some issue, such as vaccine safety or government complicity in a Big Pharma conspiracy to hype the pandemic, could easily find websites that supported their belief, websites that rebutted it, or websites that tried to assess the pros and cons neutrally.
As usual, most people relied mostly on mainstream sources – which were often misleading in other ways. But it is certainly easier than ever before to get non-mainstream viewpoints during a crisis.
9. All eyes were on the pandemic communications that came from the federal level, but did you notice anything unique or different messaging strategies that surfaced at the state or local level?
It is important to notice how few state or local health authorities deviated from the federal line with regard to messaging. The CDC sent out frequent lists of key messages, and most state and local health officials gratefully treated them as marching orders. Legally, most public health decision-making power is in state and local hands, and the CDC is just advisory. In practice during the pandemic, the CDC’s recommendations functioned as commands, sometimes for better and sometimes for worse.
On the swine flu vulnerability of different age groups, hundreds of state and local officials routinely upgraded the CDC’s misleading but linguistically accurate messages into overtly incorrect factual claims. For example, the CDC’s vaccine advisory committee recommended priority H1N1 vaccination for children up to age 18 because they are in “close contact with each other in school and day care settings, which increases the likelihood of disease spread,” and for young adults 19-24 because “they often live, work, and study in close proximity, and they are a frequently mobile population” – true statements. But states would then issue press releases like one from Vermont claiming that “college students were among the priority groups identified as being most at risk for serious illness from the flu,” which was not true.
As late as January 2010, New York City Health Commissioner Thomas Farley issued a press release stating that “People in priority groups are at higher risk of hospitalization and death if they get sick. So don’t take the risk – get the vaccine today.” This was partly true: Children aged 0–4 had the highest H1N1 hospitalization rate. And it was partly false: Children aged 0–4 had the lowest H1N1 death rate; the death rate for the “priority group” that included everyone under age 25 was lower by far than the death rate for all age groups 25 and up.
Several of our answers address the controversy (or what should be a controversy) over the age-specific H1N1 death rates, and how officials have misrepresented these death rates. You can see the CDC graph of the death rates by age group at: http://www.cdc.gov/H1N1flu/images/graphs/GraphC.gif. Here it is, pasted in from that site.
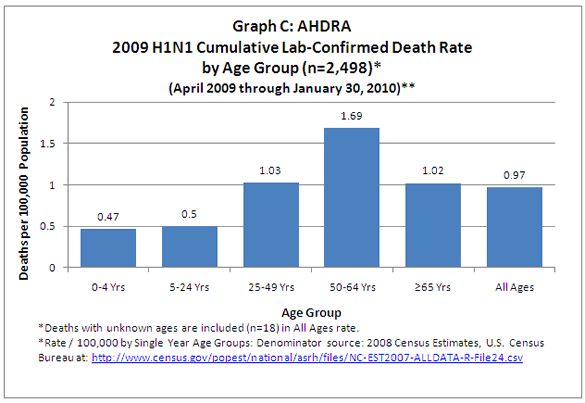{kind=link}
We interviewed a number of state and local officials about these sorts of discrepancies. Most said they hadn’t been aware of the actual data on the CDC website (and in some cases on their own websites). They were passing along the impression they got from the weekly CDC conference calls about the severe risk to kids and young adults. They all emphasized how swamped they were with their H1N1 response, and how grateful they were to the CDC for providing talking points for state and local messaging. Several were shocked when we directed them to death rate data on the CDC website, which completely contradicted the impression they had earnestly passed along to their publics.
But some state and local officials were aware of the data, and of the contradictions between the data and the messaging. They nonetheless transmitted the misleading or inaccurate messages. Each of us had several conversations with state and local health communicators and even high-ranking health officials that took the following form: “Why are you saying X?” “That’s what the CDC is saying.” “But you know it’s a mistake. You just told me so.” “We can’t say something different from what the CDC is saying.”
Copyright © 2010 by Peter M. Sandman and Jody Lanard